Collaborating on Mobile Health Tools with Balsamiq

 Dustin Dunsmuir and Luisa Flohr work on the Pediatric Anesthesia Research Team (PART) at the British Columbia Children's Hospital.
Dustin Dunsmuir and Luisa Flohr work on the Pediatric Anesthesia Research Team (PART) at the British Columbia Children's Hospital.
PART has developed inexpensive and easy to use mobile health tools focusing on preventing and monitoring pre-eclampsia in low and middle income areas. Their motivation is simple: according to the World Health Organization, as stated on the "PRE-EMPT" website (one of Dustin's projects), pre-eclampsia is "the second leading cause of maternal death, and results in 60,000-80,000 maternal deaths each year," with over 99% of these deaths occurring in low and middle income countries.
Here is the coordinator of the Community Level Interventions for Pre-eclampsia (CLIP) project talking about how it came about:
For this specific project, PART collaborated with PRE-EMPT investigators to create a mobile application called "Pre-eclampsia Integrated Estimate of RiSk on the Move (PotM)" to assess pre-eclampsia risk in areas without formal health care systems. The target audience is community health workers, many of whom have limited experiences with mobile technology.
They used wireframes created with Balsamiq to do usability testing and participatory design with representative users before and after development.
According to a paper they published in JMIR mHealth and uHealth, this approach was validated by the following conclusion:
By including target end-users in the design and evaluation of PotM, we have developed an app that can be easily integrated into health care settings in low- and middle-income countries.
Q&A with Dustin and Luisa
What industry do you work in, and what is your title or job description?
Dustin Dunsmuir: I’m a software developer in the Pediatric Anesthesia Research Team at the BC Children’s Hospital. We create technology, including mHealth solutions, which optimize and improve clinical care at the hospital and in global health projects. The largest clinical trial I have provided an app for is the Community-Level Interventions for Pre-eclampsia trial, involving over 75,000 pregnant women.
Luisa Flohr: I am a pediatrics resident, and between training positions I am working as a research assistant, also for the Pediatric Anesthesia Research Team. In this position, I am helping to develop a mobile application to support team decision-making and communication for the intensive care unit.


Early wireframes for designing the clinical Signs page for the CLIP trial. (read the paper here.)
What kinds of things are you excited about in your industry?
DD: The ubiquity of mobile phones and ever increasing presence of smartphones, even in low-income countries, combined with the development of new inexpensive sensors has the potential to transform clinical care. We can provide easy to use diagnostic mHealth applications that combine demographics and vital signs sensor data and provide a clinical recommendation. For example, an app can tell a community healthcare worker whether a pregnant woman needs to go to the hospital or inform a hospital nurse whether a child being discharged from the hospital has a high risk of mortality.
These decisions can be made on more than just the user’s training, but also based on expert opinion and the outcomes of thousands of previous patients. Apps can also track a patient’s health over time and reduce hospital visits by providing remote communication between patient and doctor.
LF: In general, the health sector is evolving quickly. We are increasingly trying to base more of our clinical decisions on evidence, such as past data and statistical analyses, to find out which interventions truly work and which do not. Powerful handheld devices such as smartphones and tablets, that are widely available, cannot only be used to reduce unnecessary or harmful treatments but also provide access to clinical information.
There is a great number of data sources in a clinical environment, but they are often difficult to access for health care team members. Compiling data and displaying it in a user-friendly way can improve clinical decision making immensely.
What suggestions do you have for someone looking to succeed in your role or industry?
DD: Take the time to produce a high quality, robust product. Mobile health is a quickly growing field, but also one where many apps are not frequently used. Apps, which are not based on clinical data are often not accepted by the users. mHealth apps, like any medical treatment, should be proven to be effective, such as through a clinical trial comparing the app to the previous gold standard method of care.
Your app also needs to serve a specific user group, which will mostly likely mean being integrated within their existing practices; thus they need to participate in its development. Questions to answer include: “Will the app be accepted by the community?”, “How will the app connect to existing systems?” and “How will the app reduce the users’ current workload?”
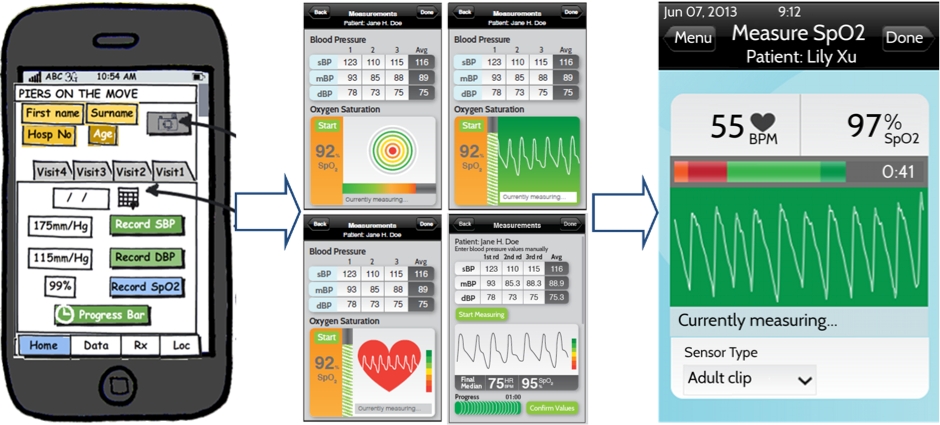 The wireframe-to-code progression for one of their apps.
The wireframe-to-code progression for one of their apps.
LF: To make a product for a specific group of users requires their immediate feedback. That is especially important for clinicians. Their work is already complicated and busy enough, a product designed to support them but that eventually creates an even higher workload or doesn't fit their workflows and mental models well will fail.
DD: If your app includes medical advice then the development process may be much more extensive, depending on where your users live. To include medical advice in an app, especially ones that connect to the patient via sensors, some countries require meeting strict regulations with carefully documented design processes.
Why and how do you use Balsamiq Mockups?
DD: Once we have an initial specifications document of initial app requirements, we jump into Balsamiq to put together a mockup of the app screens. The intuitive drag and drop method of laying out a page makes for a fast prototyping cycle. Linking the pages together and exporting a PDF that navigates like a real app (buttons go to other screens) means we can easily send this from Vancouver, Canada to collaborators and end-users, whether they are in Pakistan or Uganda, and obtain their feedback on content and navigation.
From this, we produce another round of mockups or potentially go back to the specifications document, as our users may not have realized something was missing until they walked through the mockup. During this process, there’s no need for users to install any special software on their computers and all prototyping can happen before any programming begins. Just as we reuse code for similar apps, we can start our mockups by opening a previous Balsamiq mockup, and edit it.
LF: The current project I am working on is a Pediatric Intensive Care Unit mobile monitoring app. Starting with an existing prototype I worked my way through the designs and improved them based on our observations and interviews of clinical staff. I created a big file for the whole application and broke it down into specific tasks. This approach allows you to strip away, or add features quickly, creating alternative versions and drag and drop layouts from other projects, potentially even with the end-user present.
The PDF export option is extremely useful because it allows the user to interact with the mockup and therefore, to spot flaws or observe actions that show when a design is not intuitive to use. This way you can improve your mockup before going through all the work of developing the software for the actual application, which is also quite cost effective.


Layouts for the Pediatric Intensive Care Unit (PICU) mobile monitoring device – VitalPAD. (read the paper here.)
Do you have any feature ideas or suggestions for how we can improve our product(s)?
DD: In older versions of Balsamiq, it was difficult to deal with all the small tabs of individual pages and to open all of these. Now, with the introduction of Projects, everything is easier to manage.
LF: I really enjoy working with the program and I think it is easy to use. However, I have some suggestions for small improvements: At times I would have needed more options for colour. The current app I am working on might need shades of certain colours or greyed out versions which is sometimes hard to create. Also, you cannot change the size or font within the same text area; you need a new box should you need to add emphasis, e.g. a bold line. (Editor's note: It's not immediately obvious, but you can format text within a text area using these formatting syntax codes.)
What challenges did you face in this project and how did you deal with them? What would you do differently next time?
DD: One of the challenges that I have faced in making apps for community healthcare workers who may never have used a smartphone or even a computer is to design an interface that they will find easy to use. Something that seems quite straightforward to me, and which matches many apps out there, may not be as intuitive to them.
For example, first time smartphone users have trouble clicking small buttons, so it was a good idea to make buttons large. Although it takes up more space, I have also opted for checkboxes or radio buttons instead of dropdown menus, because then all options are visible immediately and it looks much more like a paper form.
LF: My project is still in the early stages, but my biggest challenge is definitely trying to think of a design from a practical point of view. The possibilities are endless; you have to be careful to stick to the user's needs because the application needs to be integrated into their workflow. I had to learn to let go of ideas I really loved because they were simply not useful or made the application too complicated. For example, we thought of adding artificial horizons to indicate whether vital parameters are within normal limits, but our clinicians told us they would not use those and prefer to see the actual numbers and graphs.
You need to listen very carefully when you get feedback and write everything down, because I know now that trying to remember what someone said retrospectively is almost impossible.
Thank you, Dustin, Luisa, and your teammates, for the important work you do! Keep it up!
Do you have a story to share about the awesome things you do with Balsamiq? Send an email to champions@balsamiq.com with your stories or blog posts!



